Skin Involvment
Approximately two-thirds of people with lupus will develop
some type of skin disease. Skin disease in lupus can cause rashes or sores (lesions), most of which will appear on sun-exposed areas, such as your face, ears, neck, arms, and legs. In addition, 40-70 percent of people with systemic lupus will find that their disease is made worse by exposure to ultraviolet (UV) rays from sunlight or artificial light.
Lupus skin disease, called cutaneous lupus erythematosus, can occur in one of three forms: chronic cutaneous (discoid) lupus erythematosus, subacute cutaneous lupus erythematosus, and acute cutaneous lupus erythematosus. Lupus skin rashes and lesions should be treated by a dermatologist, a physician who specializes in caring for the skin. To determine whether a lesion or rash is due to cutaneous lupus, your physician will usually want to look at the tissue under a microscope. Taking the tissue sample is called a biopsy.
The Forms of Cutaneous Lupus
Chronic cutaneous lupus (discoid lupus) appears as
disk-shaped, round lesions. The sores usually appear on your scalp and face,
but sometimes they will occur on other parts of your body as well.
Approximately 10 percent of people with discoid lupus later develop systemic
lupus, but these people probably had systemic lupus to begin with, with the
skin rash as the first symptom.
Discoid lupus lesions are often red, scaly, and thick. Usually
they do not hurt or itch. Over time these lesions can produce scarring and skin
discoloration (darkly colored and/or lightly colored areas). Discoid lesions
that occur on your scalp may cause your hair to fall out. If the lesions form
scars when they heal, your hair loss may be permanent. Cancer can develop in
discoid lesions that you have had for a long time, so tell your doctor about
any changes in the appearance of one of these lesions.
Discoid lupus lesions can be very photosensitive, so
preventive measures are important:
scaly skin with distinct edges, or as red, ring-shaped lesions. The lesions
occur most commonly on the sun-exposed areas of your arms, shoulders, neck, and
body. The lesions usually do not itch or scar, but they can become discolored.
Subacute cutaneous lesions are also photosensitive so preventive measures
should be taken when spending time outdoors or under fluorescent
lights.
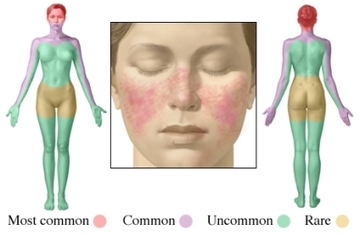
Acute cutaneous lupus lesions occur when your systemic lupus is active.
The most typical form of acute cutaneous lupus is a malar rash -- flattened
areas of red skin on your face that resemble a sunburn.
When the rash appears on both cheeks and across the bridge of the nose in the
shape of a butterfly, it is known as the "butterfly rash." However, the rash
can also appear on your arms, legs, and body. These lesions tend to be very
photosensitive. They typically do not produce scarring, although changes in
skin color may occur.
Other Skin Problems
There are several other conditions that can occur when you
have lupus:
Calcinosis is caused by a buildup of calcium deposits
under your skin. These deposits can be painful, and may leak a white liquid.
Calcinosis can develop from a reaction to steroid injections or as a result of
kidney failure.
Cutaneous vasculitis lesions occur when inflammation
damages the blood vessels in your skin. The lesions typically appear as small,
red-purple spots and bumps on the lower legs; occasionally, larger knots
(nodules) and ulcers can develop. Vasculitis lesions can also appear in the
form of raised sores or as small red or purple lines or spots in your
fingernail folds or on the tips of your fingers. In some cases cutaneous
vasculitis can result in significant damage to skin tissue. Areas of dead skin
can appear as sores or small black spots at the ends of your fingers or around
your fingernails and toes, causing gangrene (death of soft tissues due to loss
of blood supply).
Hair loss can occur for other reasons besides scarring
on the scalp. Severe systemic lupus may cause a temporary pattern of hair loss
that is then replaced by new hair growth. A severe lupus flare can result in
fragile hair that breaks easily. Such broken hairs at the edge of your scalp
give a characteristic ragged appearance termed "lupus hair."
Raynaud’s phenomenon is a condition in which the blood
vessels in your hands and feet go into spasm, causing restricted blood flow.
Lupus-related Raynaud’s usually results from inflammation of nerves or blood
vessels and most often happens in cold temperatures, causing the tips of your
fingers or toes to turn red, white, or blue. Pain, numbness, or tingling may
also occur. If you have Raynaud’s phenomenon try to avoid cold conditions, and,
if necessary, wear gloves or mittens and thick socks when in an air-conditioned
area.
Livedo reticularis and palmar erythema are
caused by abnormal rates of blood flow through your capillaries and small
arteries. You will have a bluish, lacelike mottling under your skin, especially
on your legs, that gives a "fishnet" appearance. Like Raynaud’s phenomenon,
these conditions tend to be worse in cold weather.
Mucosal ulcerations are sores in your mouth or nose or,
less often, in lining of vaginal tissue. These ulcers can be caused by both
cutaneous lupus and systemic lupus. It is important to differentiate lupus
ulcers from herpes lesions or cold sores, which may be brought on by the use of
immunosuppressive drugs. Lupus ulcers are usually painless and signs of
inflammation will show up in the biopsy.
Petechiae (pah-TEE-kee-eye) are tiny red spots on your
skin, especially on the lower legs, that result from low numbers of platelet in
your blood, a condition called thrombocytopenia. Although thrombocytopenia is
common in lupus, serious bleeding as a result of the low number of platelets
usually does not occur.
Treating Cutaneous Lupus
The medication used to treat lupus-related skin conditions
depends on what kind of cutaneous lupus you have. The most common treatments
are ointments, such as steroid cream or gel. In some cases liquid steroids will
be injected directly into the lesions.
A new class of drugs, called topical immuno-modulators, has
been developed to treat serious skin conditions without the side effects found
in corticosteroids: both tacrolimus ointment (Protopic®) and pimecrolimus cream
(Elidel®) have been shown to suppress the activity of the immune system in the
skin, including the butterfly rash, subacute cutaneous lupus, and possibly even
discoid lupus lesions.
In addition, thalidomide (Thalomid®) has been increasingly
accepted as a treatment for the types of lupus that affect the skin; it has
been shown to greatly improve cutaneous lupus that has not responded to other
treatments.
Treatments for Cutaneous Lupus
Preventative Treatments
Systemic Treatments for Mild to Moderate Disease
FDA-approved for cutaneous lupus.
This information comes from the Lupus Foundation of America.
some type of skin disease. Skin disease in lupus can cause rashes or sores (lesions), most of which will appear on sun-exposed areas, such as your face, ears, neck, arms, and legs. In addition, 40-70 percent of people with systemic lupus will find that their disease is made worse by exposure to ultraviolet (UV) rays from sunlight or artificial light.
Lupus skin disease, called cutaneous lupus erythematosus, can occur in one of three forms: chronic cutaneous (discoid) lupus erythematosus, subacute cutaneous lupus erythematosus, and acute cutaneous lupus erythematosus. Lupus skin rashes and lesions should be treated by a dermatologist, a physician who specializes in caring for the skin. To determine whether a lesion or rash is due to cutaneous lupus, your physician will usually want to look at the tissue under a microscope. Taking the tissue sample is called a biopsy.
The Forms of Cutaneous Lupus
Chronic cutaneous lupus (discoid lupus) appears as
disk-shaped, round lesions. The sores usually appear on your scalp and face,
but sometimes they will occur on other parts of your body as well.
Approximately 10 percent of people with discoid lupus later develop systemic
lupus, but these people probably had systemic lupus to begin with, with the
skin rash as the first symptom.
Discoid lupus lesions are often red, scaly, and thick. Usually
they do not hurt or itch. Over time these lesions can produce scarring and skin
discoloration (darkly colored and/or lightly colored areas). Discoid lesions
that occur on your scalp may cause your hair to fall out. If the lesions form
scars when they heal, your hair loss may be permanent. Cancer can develop in
discoid lesions that you have had for a long time, so tell your doctor about
any changes in the appearance of one of these lesions.
Discoid lupus lesions can be very photosensitive, so
preventive measures are important:
- avoid being out in the sunlight between the hours of 10 a.m.
and 4 p.m. - use plenty of sunscreen when you are outdoors
- wear sun-protective clothing and broad-brimmed hats
- limit the amount of time you spend indoors under fluorescent
lights
scaly skin with distinct edges, or as red, ring-shaped lesions. The lesions
occur most commonly on the sun-exposed areas of your arms, shoulders, neck, and
body. The lesions usually do not itch or scar, but they can become discolored.
Subacute cutaneous lesions are also photosensitive so preventive measures
should be taken when spending time outdoors or under fluorescent
lights.
Acute cutaneous lupus lesions occur when your systemic lupus is active.
The most typical form of acute cutaneous lupus is a malar rash -- flattened
areas of red skin on your face that resemble a sunburn.
When the rash appears on both cheeks and across the bridge of the nose in the
shape of a butterfly, it is known as the "butterfly rash." However, the rash
can also appear on your arms, legs, and body. These lesions tend to be very
photosensitive. They typically do not produce scarring, although changes in
skin color may occur.
Other Skin Problems
There are several other conditions that can occur when you
have lupus:
Calcinosis is caused by a buildup of calcium deposits
under your skin. These deposits can be painful, and may leak a white liquid.
Calcinosis can develop from a reaction to steroid injections or as a result of
kidney failure.
Cutaneous vasculitis lesions occur when inflammation
damages the blood vessels in your skin. The lesions typically appear as small,
red-purple spots and bumps on the lower legs; occasionally, larger knots
(nodules) and ulcers can develop. Vasculitis lesions can also appear in the
form of raised sores or as small red or purple lines or spots in your
fingernail folds or on the tips of your fingers. In some cases cutaneous
vasculitis can result in significant damage to skin tissue. Areas of dead skin
can appear as sores or small black spots at the ends of your fingers or around
your fingernails and toes, causing gangrene (death of soft tissues due to loss
of blood supply).
Hair loss can occur for other reasons besides scarring
on the scalp. Severe systemic lupus may cause a temporary pattern of hair loss
that is then replaced by new hair growth. A severe lupus flare can result in
fragile hair that breaks easily. Such broken hairs at the edge of your scalp
give a characteristic ragged appearance termed "lupus hair."
Raynaud’s phenomenon is a condition in which the blood
vessels in your hands and feet go into spasm, causing restricted blood flow.
Lupus-related Raynaud’s usually results from inflammation of nerves or blood
vessels and most often happens in cold temperatures, causing the tips of your
fingers or toes to turn red, white, or blue. Pain, numbness, or tingling may
also occur. If you have Raynaud’s phenomenon try to avoid cold conditions, and,
if necessary, wear gloves or mittens and thick socks when in an air-conditioned
area.
Livedo reticularis and palmar erythema are
caused by abnormal rates of blood flow through your capillaries and small
arteries. You will have a bluish, lacelike mottling under your skin, especially
on your legs, that gives a "fishnet" appearance. Like Raynaud’s phenomenon,
these conditions tend to be worse in cold weather.
Mucosal ulcerations are sores in your mouth or nose or,
less often, in lining of vaginal tissue. These ulcers can be caused by both
cutaneous lupus and systemic lupus. It is important to differentiate lupus
ulcers from herpes lesions or cold sores, which may be brought on by the use of
immunosuppressive drugs. Lupus ulcers are usually painless and signs of
inflammation will show up in the biopsy.
Petechiae (pah-TEE-kee-eye) are tiny red spots on your
skin, especially on the lower legs, that result from low numbers of platelet in
your blood, a condition called thrombocytopenia. Although thrombocytopenia is
common in lupus, serious bleeding as a result of the low number of platelets
usually does not occur.
Treating Cutaneous Lupus
The medication used to treat lupus-related skin conditions
depends on what kind of cutaneous lupus you have. The most common treatments
are ointments, such as steroid cream or gel. In some cases liquid steroids will
be injected directly into the lesions.
A new class of drugs, called topical immuno-modulators, has
been developed to treat serious skin conditions without the side effects found
in corticosteroids: both tacrolimus ointment (Protopic®) and pimecrolimus cream
(Elidel®) have been shown to suppress the activity of the immune system in the
skin, including the butterfly rash, subacute cutaneous lupus, and possibly even
discoid lupus lesions.
In addition, thalidomide (Thalomid®) has been increasingly
accepted as a treatment for the types of lupus that affect the skin; it has
been shown to greatly improve cutaneous lupus that has not responded to other
treatments.
Treatments for Cutaneous Lupus
Preventative Treatments
- Avoidance/protection from sunlight and artificial ultraviolet
light - Seek shade
- Sunscreens -- physical and chemical
- Corticosteroid creams, ointments, gels, solutions, lotions,
sprays, foams - Calcineurin inhibitors
- tacrolimus ointment (Protopic®)
- pimecrolimus cream (Elidel®)
Systemic Treatments for Mild to Moderate Disease
- Corticosteroids -- short term
- Antimalarials
- hydroxychloroquine (Plaquenil®)
- chloroquine (Aralen®)
- quinacrine (available from compounding pharmacies only)
- Retinoids
- synthetic forms of vitamin A—isotretinoin (Accutane®),
acitretin (Soriatane®)
- synthetic forms of vitamin A—isotretinoin (Accutane®),
- Sulfones
- diaminodiphenylsulfone
(Dapsone®)
- diaminodiphenylsulfone
- Corticosteroids -- long term
- Gold
- oral—auronofin (Ridura®)
- intramuscular—gold sodium thiomaleate (Myochrisine®)
- Thalidomide (Thalomid®)
- Methotrexate
- Azathioprine (Imuran®)
- Mycophenolate mofetil (CellCept®)
- Biologics
- efalizumab (Raptiva®)
FDA-approved for cutaneous lupus.
This information comes from the Lupus Foundation of America.
